Post-Acute Care · Three Patents Pending
Care doesn't stop
at discharge.
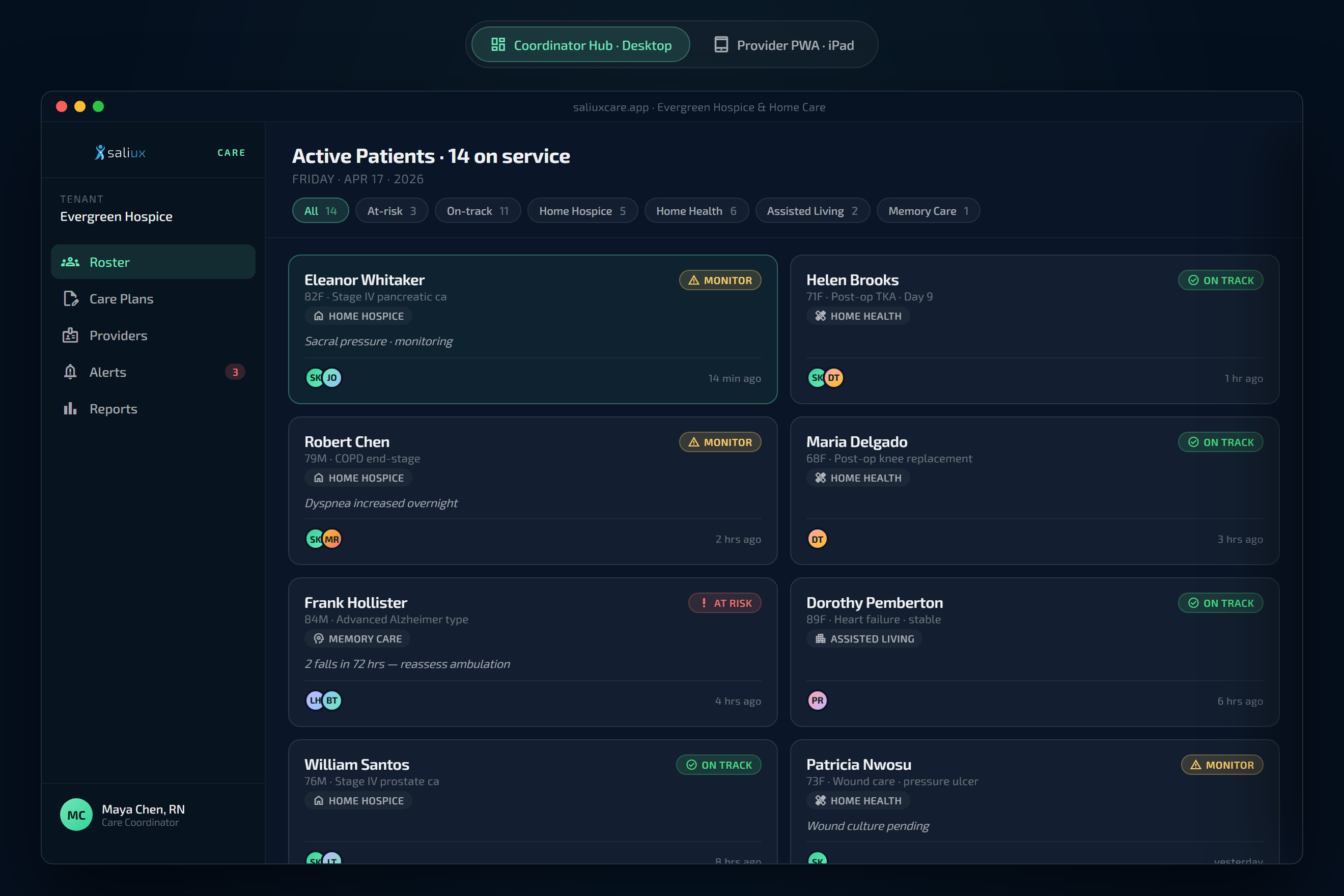
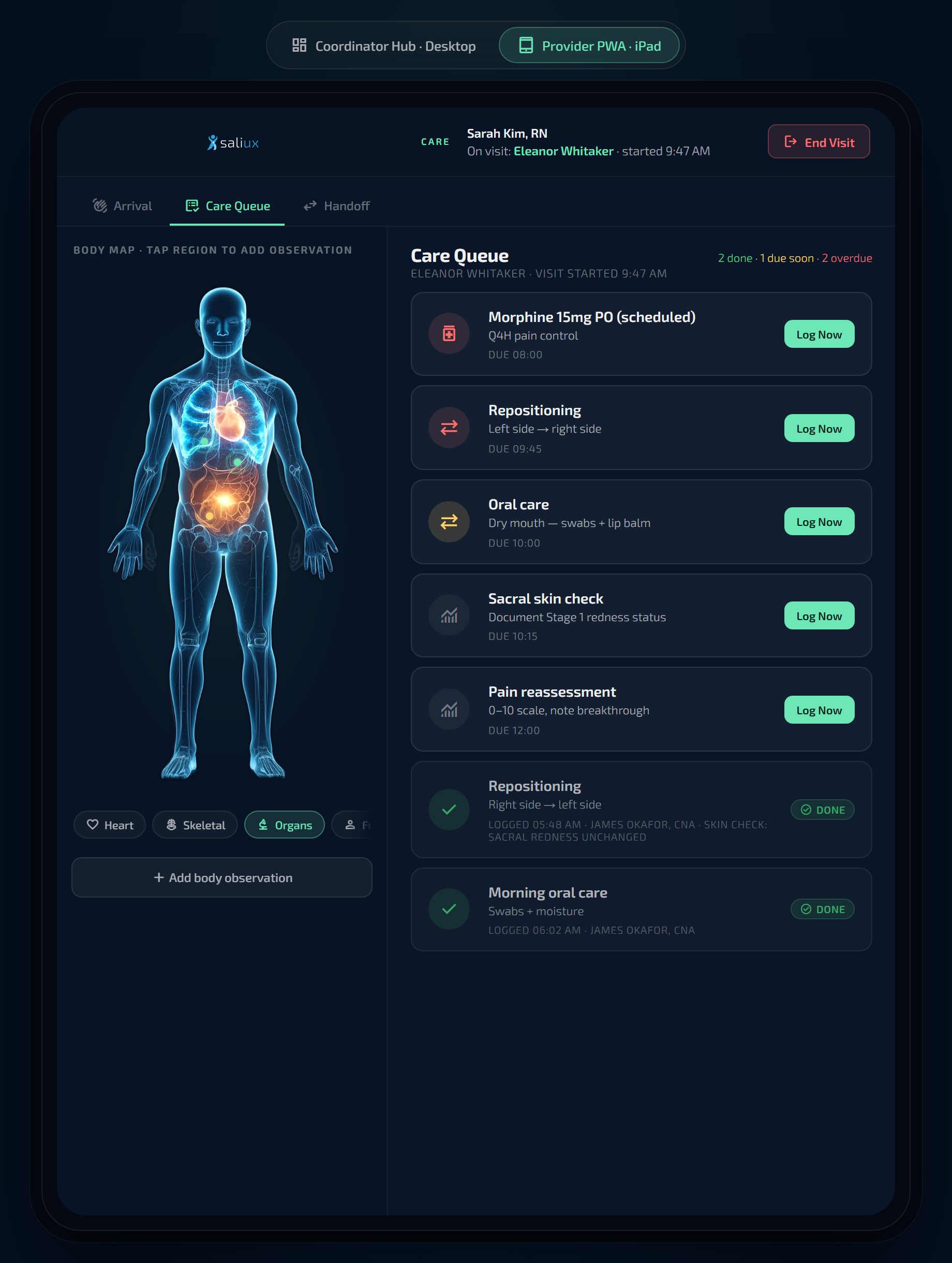
The care the hospital assembled during an admission — conditions, medications, open obligations, wound care protocols — doesn't disappear when the patient walks out. And for home care agencies whose patients self-provision the record from home, Saliux Care stands alone on the same FHIR spine. Either path. One coordination layer. In real time.